 |
| Week 30 Severe Influenza - HK Influenza Express |
#12,652
Flu levels are still high in Hong Kong - and likely to remain so for several more weeks - but after nearly 3 months of steady growth the number of reported flu cases has begun to decline. This unusually severe summer flu season - which began in early May - has claimed more than 300 lives over the past 90 days.
Hong Kong is known for having a biphasic or `double peaked’ flu season, but their heaviest activity usually occurs between February and April with a less severe season in mid to late summer (see Seasonality of Influenza A(H3N2) Virus: A Hong Kong Perspective (1997–2006).
We've two reports. Our usual weekly Flu Express and a flu-centric edition of Hong Kong's Bi-weekly Communicable Diseases Watch (CDW).First, an overview of this summer's flu season from today's CDW.
Updated Situation of Seasonal Influenza in Hong Kong
Reported by Ms Vera CHOW, Scientific Officer, Respiratory Disease Office, Surveillance and Epidemiology Branch, CHP
(Excerpt)
Discussion
The local seasonal influenza activity has been atypical in 2017.The winter season was mild with low level of influenza circulation yet the influenza activity in the summer season was much higher than that recorded in the winter season in 2017. It was also higher than previous summer seasons. Similar to Hong Kong, sharp increases in influenza activity have also been recorded in June and July 2017 in Guangdong and Macau.
Several factors might account for the severity of this season. This season was predominated by influenza A(H3N2) virus, which is notoriously known to affect the elderly population. The aging population in Hong Kong has resulted in an increasing number of frail elderly who are more prone to influenza infection and its complications. There was a net increase of 183 300 persons aged 65 years or above between 2012 and 2016.The annual increase in population size of 65 years or above was more than 4% in the past five years in Hong Kong. Furthermore, the immunity induced by seasonal influenza vaccination in late 2016 has been waning in the elderly population, making them susceptible to influenza infection in the current summer season.
The latest surveillance data suggested that the peak of this season has already passed though the influenza activity still remained at a high level. In the past three winter seasons (2014, 2015 and 2016) with high influenza activity recorded, the duration ranged from 16 to 17 weeks. It took 10 to 13 weeks for the influenza activity to decrease from the peak level back to the baseline. So far, about 13 weeks have passed in this season. It is foreseen that it will last for some time before the influenza activity returns to the baseline. CHP will closely monitor the situation
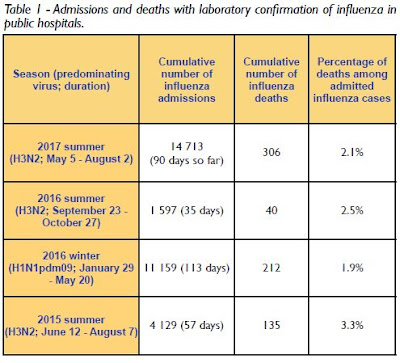
The following CDW chart compares the severity of this summers heavy flu season with other Hong Kong flu seasons since the summer of 2015.
From this week's Flu Express.
FLU EXPRESS
Flu Express is a weekly report produced by the Respiratory Disease Office of the Centre for Health Protection. It monitors and summarizes the latest local and global influenza activities.
Local Situation of Influenza Activity (as of Aug 2, 2017)
Reporting period: Jul 23 – 29, 2017 (Week 30)
(SNIP)
- The latest surveillance data showed that the local influenza activity has decreased in the past week but still remained at a high level. It is foreseen that the influenza activity will remain at a high level in the coming weeks.
- The Centre for Health Protection (CHP) has collaborated with the Hospital Authority (HA) and private hospitals to reactivate the enhanced surveillance for severe seasonal influenza cases (i.e. influenza-associated admissions to intensive care unit or deaths) among patients aged 18 or above since May 5, 2017. As of Aug 2, 431 severe cases (including 304 deaths) were recorded. Separately, 19 cases of severe paediatric influenza-associated complication/death (including three deaths) (aged below 18 years) were recorded in the same period.
- Apart from adopting personal, hand and environmental hygiene practices against respiratory illnesses, those members of the public who have not received influenza vaccine may get the vaccination as soon as possible for personal protection.
Surveillance of severe influenza cases
(Note: The data reported are provisional figures and subject to further revision)
Since the activation of the enhanced surveillance for severe influenza infection on May 5, 2017, a total of 450 severe cases (including 307 deaths) were recorded cumulatively (as of Aug 2) (Figure 9). These included:
Enhanced surveillance for severe seasonal influenza (Aged 18 years or above)
- 431 cases (including 304 deaths) among adult patients aged 18 years or above. Among them, 385 patients had infection with influenza A(H3N2), 21 patients with influenza A(H1N1)pdm09, 13 patients with influenza B and 12 patients with influenza A pending subtype. 160 (37.1%) were known to have received the influenza vaccine for the 2016/17 season. Among the 304 fatal cases, 137 (45.1%) were known to have received the influenza vaccine. In the winter season in early 2017, 66 adult severe cases (including 41 deaths) were filed.
- 19 cases (including three deaths) of severe paediatric influenza-associated complication/ death. Seventeen (89.5%) cases did not receive the influenza vaccine for the 2016/17 season. To date in 2017, 27 paediatric cases (including four deaths) were filed.
Surveillance of severe paediatric influenza-associated complication/death (Aged below 18 years)
- In week 30, 71 cases of influenza associated ICU admission/death were recorded (including 54 deaths), which was higher than 65 cases (including 39 deaths) recorded in week 28. In the first 4 days of week 31 (Jul 30 to Aug 2), 36 cases of influenza associated ICU admission/death were recorded, in which 25 of them were fatal.
(Continue .. . )
- There was one case of severe paediatric influenza-associated complication each in week 30 and the first 4 days of week 31 (Jul 30 to Aug 2).
Taiwan reported that their unusual summer flu surge had peaked a couple of weeks ago (see Taiwan's Summer H3N2 Epidemic Continues Near Peak), and while getting solid information from the Chinese mainland has been difficult, today's Flu Express does report:
- In Southern China (week ending Jul 23, 2017), influenza activity was at the summer peak and continued to increase. The proportion of ILI cases in emergency and outpatient departments reported by sentinel hospitals was 4.1%, lower than that reported in the previous week (4.3%), but higher than that in the corresponding period in 2014-2016 (3.6%, 3.6%, 3.1%). The proportion of influenza detections was 21.0%, higher than 18.3% recorded in the previous week. Influenza A (H3N2) constituted 90.3% of the influenza detections.
- In Macau (week ending Jul 22, 2017), the proportion of ILI cases among both adults and children in emergency departments increased from the previous week. The proportion of influenza detections was 53.6%, higher than 44.9% in the previous week. Influenza A(H3) constituted 82.3% of the influenza detections.
Meanwhile, the winter flu season in Australia continues to gain momentum, with their latest DOH surveillance report stating:
Australian Influenza Surveillance Report No 05 - 08 July to 21 July 2017
Summary
- Influenza activity at the national level continued to increase this reporting fortnight indicating that the season is underway in a majority of regions across Australia. This increase in activity occurred approximately one month earlier than in 2016.
- Influenza was detected at increasing levels by the majority of sentinel laboratories this reporting fortnight. For the first time since reporting for 2017 began, influenza A was the most common respiratory virus detected by a majority of sentinel laboratories, followed by respiratory syncytial virus (RSV).
- Influenza A(H3N2) is currently the predominant circulating A subtype in the majority of jurisdictions. Nationally, notifications of laboratory confirmed influenza B viruses reached a plateau this reporting fortnight. Notification rates this year to date have been highest in adults aged 85 years or older, with a secondary peak in young children, aged less than 10 years.
- Influenza-like illness (ILI) in the community and ILI presentations to sentinel GPs this fortnight continued the overall increasing trend, however remain within the range of recent seasons.
Meanwhile, in New Zealand, influenza activity (week 30) remains above the baseline, but at low levels.
- Hospitalisations with confirmed influenza have increased in recent weeks in line with the seasonal increase in community level activity. To date, the seasonal influenza vaccines appear to be a good match for circulating virus strains.